I apologize for neglecting this blog for so long! The reason, and the good news, is that I had to finish Plunder and Survival: Stories of Theft, Loss, Recovery and Migration of Nazi-Uprooted Art, my fifteenth book. Bloomsbury will publish it on October 16th, 2025. It is already available for preorder!
In honor of yesterday’s important anniversary, here is a little story that will take you back by over eight decades.
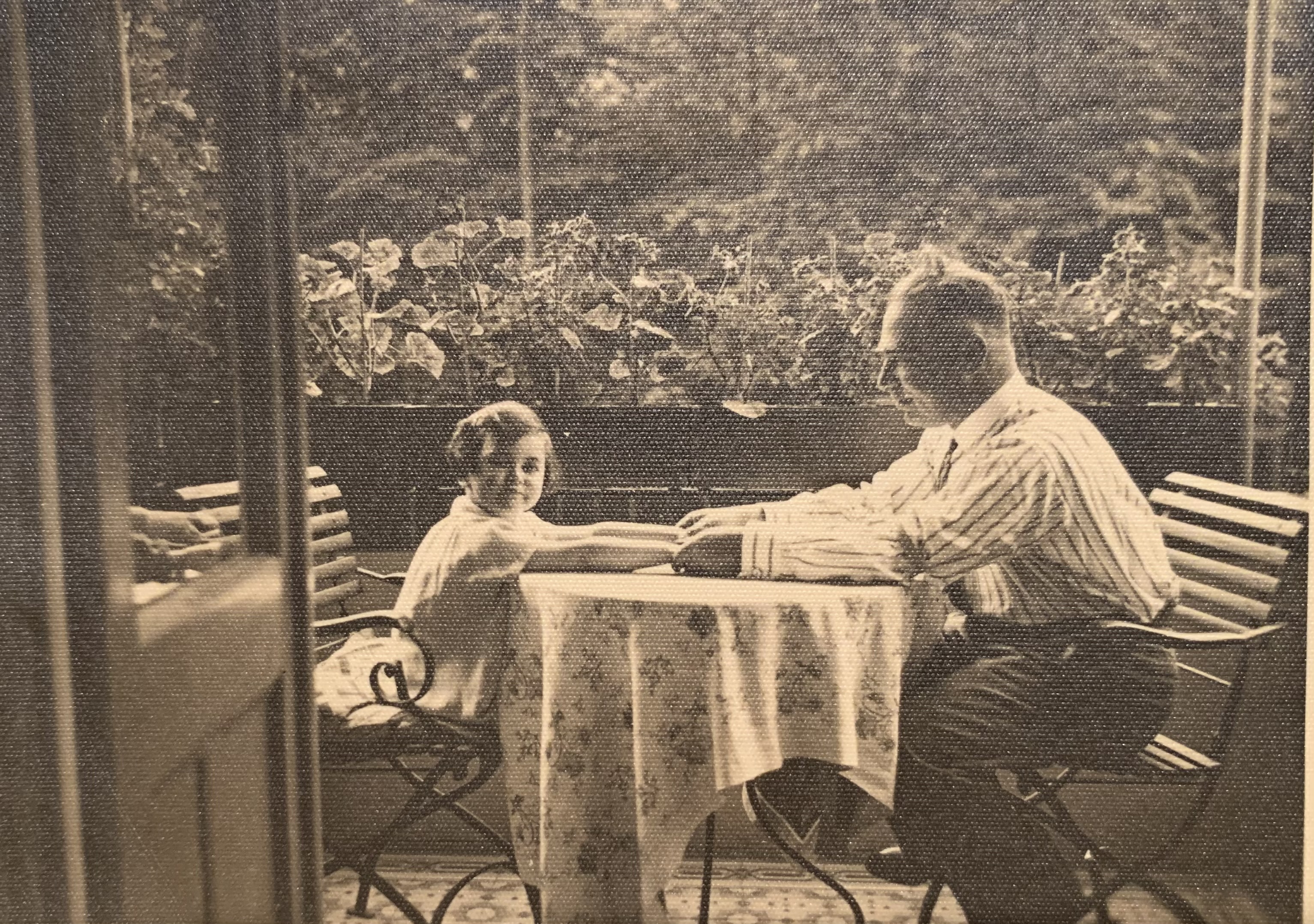
I cautiously stretch my arthritic limbs in my bed in Brooklyn. It is 5 AM: time to take my diabetes pill. Suddenly, I am wide awake. I have been transported back to 85 years ago, and my mom is standing at the door of the Brussels bedroom I share with my sister Gabrielle.
“Kinder, get up,” she says. “We may have to go to the basement.” A rumbling sound fills the room. Since when is Mutti afraid of a thunderstorm? I wonder. Then my father joins her. His face is ashen.
“The radio announced that the Germans invaded Belgium and Holland. We are at war,” he says.
I was about to turn 15, but to this day, I think of May 10th, 1940, as the day my life began.
My family of four had arrived in Belgium two years earlier, escaping Nazi rule in Germany, where my Jewish ancestors had lived for centuries. It had been hard for my parents to leave their comfortable bourgeois existence, but I blossomed in my new school’s tolerant atmosphere. My classmates looked out for me, explaining to those who were unfamiliar with my background that I needed special consideration because French was not my native tongue.
Routines often persist in spite of catastrophes. On the morning of May 10th, the local bakery had delivered our freshly baked croissants while Nazi troops invaded. Doubting the Belgian army’s ability to stave them off, our parents decided we would try to outrun the Germans.
While we did our best to savor the croissants, our doorbell rang. Two members of the Belgian Civil Service had arrived to arrest us because we were German nationals. They loaded us aboard a hastily requisitioned hearse that drove us to my beloved school, which had been turned into a makeshift detention center. Pandemonium reigned. Most adults were stunned and sat quietly on makeshift accommodations while the teens organized a ball game. Soup materialized at midday.
During the afternoon, Madame Tordeur, the school director, spotted me. For some unfathomable reason, this ordinary-looking middle-aged woman terrified me. Whenever she entered my classroom, I expected her to single me out and declare, “Suzanne Bamberger, you don’t belong here. Leave.” Now, she shook my hand, her eyes moist. Suddenly, the enormity of what had happened hit me. My sense of adventure evaporated, and I sat quietly beside my mom. Shortly thereafter, the authorities released women and children but kept my father. Two days later, he and other wrongfully arrested men were shipped to a terrible concentration camp in the south of France. We would not see my father for six years.
Famine, war, redrawn borders, and persecution or fear thereof have often forced specific groups to flee their homes. Since World War I, the number of refugees that roam the world has increased exponentially. In 1915, Armenians fled their genocidal Turkish compatriots. Soon after, “White Russians” escaped from the nascent Soviet Union. Vanquished Republican Spaniards fled Francisco Franco’s Fascist Spain, and Jews fleeing Hitler swelled their ranks. And it’s not just Europe—this kind of displacement has occurred all over the world. According to the United Nations Refugee Agency, there were 20 million refugees in 1940 and more than 120 million by mid-2024.
As I stated at a rally at Kennedy Airport when Donald Trump instituted what was known as the “Muslim ban” during his first presidency, being a refugee is not a permanent condition. Even though I spent decades as a refugee, my life has been good and successful. Still, I know being a refugee leaves a permanent imprint on the self.
When we left Germany for Belgium in 1938, my mother told me to identify myself as a “political refugee”—whatever that meant to a 12-year-old. The term became more meaningful after my father’s abrupt departure, at which point my mother had to manage, with two children, entirely on her own. Perhaps it was fortunate that she did not know she would have to do so for six long years.
She decided we would join the one million Belgian citizens—1/8th of the total population—who left their homes to avoid the Nazi occupation. Our plan was to take the train to Ostend on the Belgian coast and cross the border into France near Dunkirk. The scene at the station in Brussels was chaos. British soldiers who were arriving to assist the Belgian, Dutch and French armies disembarked as Belgian refugees fought their way aboard the few departing trains. It took us hours to squeeze aboard one, and then it took another 24 hours to cover the 67 miles to Ostend.
Miraculously, we found a room in a hotel. The next day, we took a street car that ran along the Belgian beach and finally walked to the border. We spent the next ten days trying to cross into France. We did not have the proper documents to satisfy the French border guards. We slept in the dunes. I can’t remember how we went to the bathroom or what we ate. We made lifelong friends with another German Jewish family who we had first met when we were both incarcerated at my school on the day the war started. Eventually, we realized that there was no point in reaching France. The German army had bypassed the coast and reached the interior of France by another route. Three weeks after we left, we returned to Brussels.
I will never be able to fathom how fortunate the three of us were to survive four years of Hitler’s Holocaust in Belgium. In addition to luck, it required the kindness of dozens of strangers. In May 1946, my father greeted us on a Hudson River pier in New York City. Though only 59, he seemed old and would die three years later. For him, as well as for me, the forced separation would never be healed.
I often wonder how being a refugee affected me. In many ways, it was an excellent way of growing up. I am incredibly appreciative of what I have. I am very resourceful. I am fluent in German, French, and English. I have acquired a “native” understanding of three different cultures—different from visiting as a tourist. I also feel a certain distance from my three “home” countries’ crimes: Nazism in Germany; Belgian King Leopold II’s plunder of the Congo; the genocide of the Native American population and the prolonged road to racial equality in the United States.
And at the same time: I never quite felt at home anywhere. I always spoke with an accent, and I needlessly grew up without a father. My sister, who was younger than me when all this happened, never lost her extreme sense of anxiety. I too worry. I am fearful of most authoritarian bodies like the police or the army. I panic during exams and only passed my driving test after the kind examiner reminded me that “they must have taught you how to parallel park in driving school.”
It is good that we can’t choose our life’s roadmap. But I am afraid that refugee problems, like climate change, poverty, epidemics, and dictatorships, are likely to stay with us.